Part of our complete guide to Ptosis (Droopy Eyelid) — this page covers Marcus Gunn jaw-wink ptosis in depth.
Marcus Gunn Jaw Wink
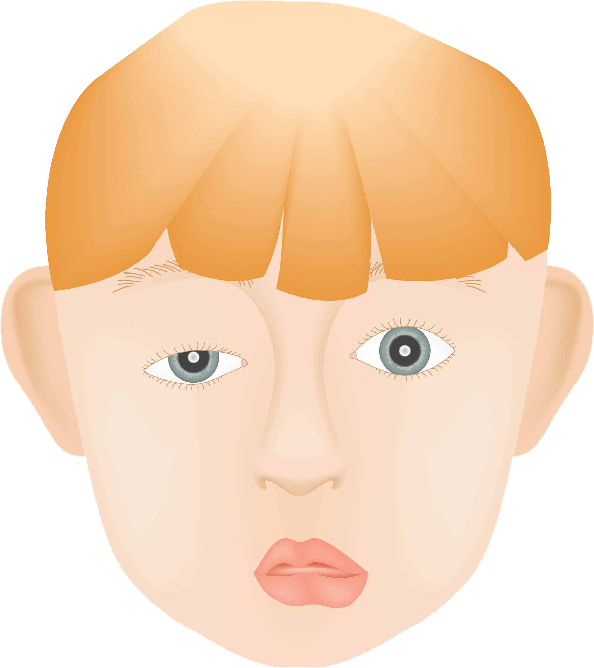
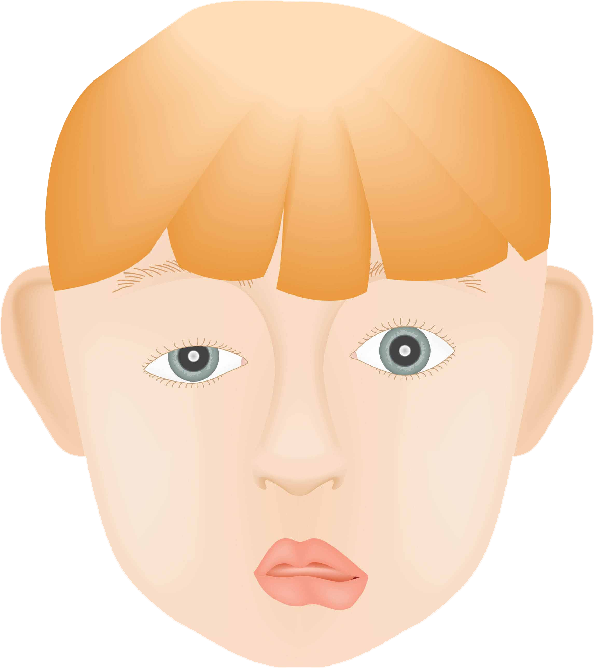
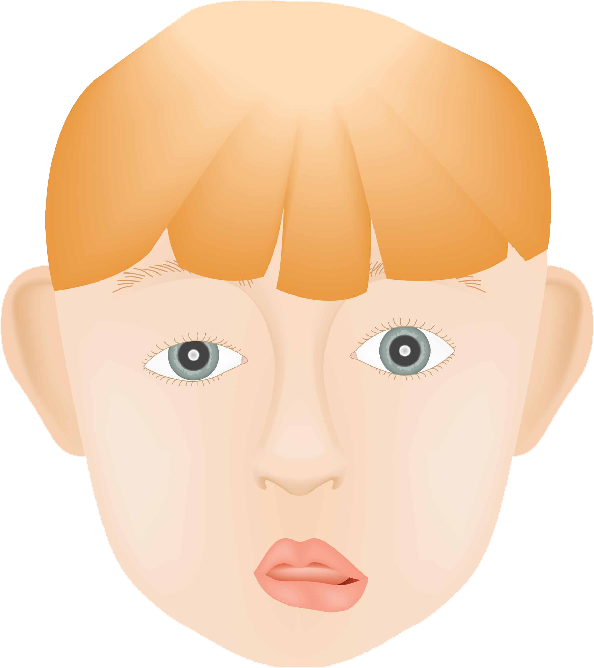
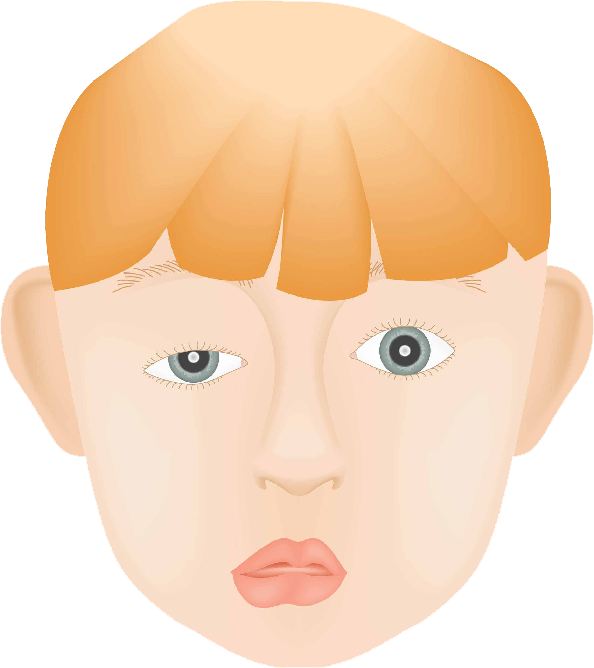
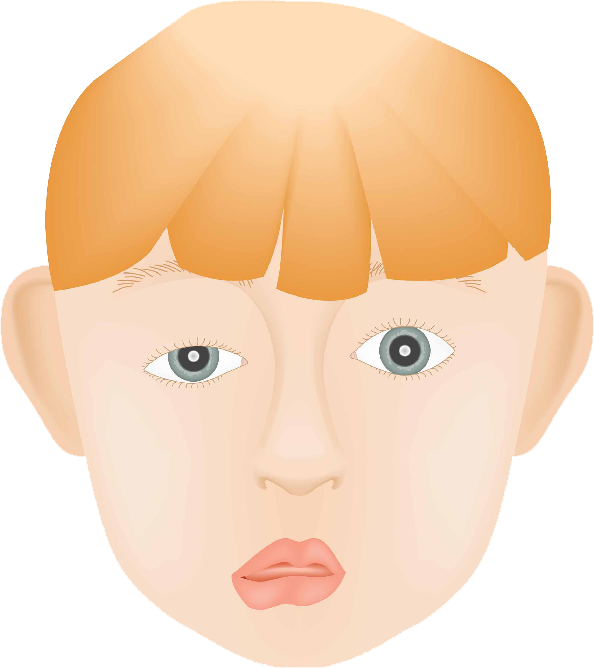
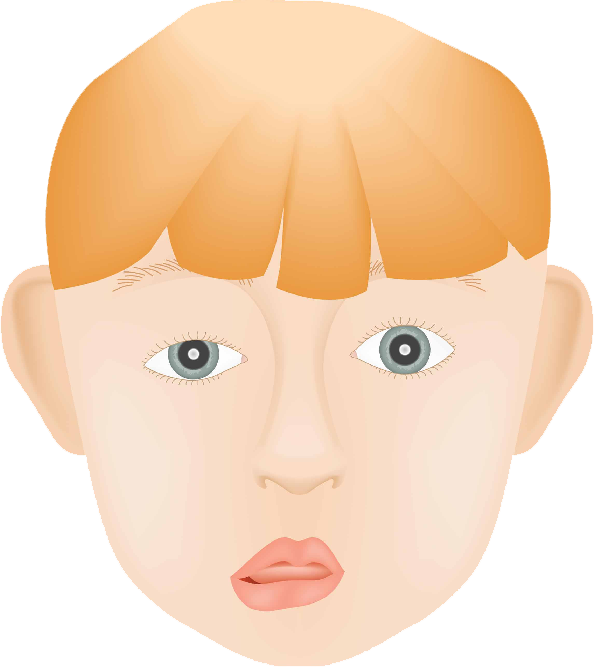
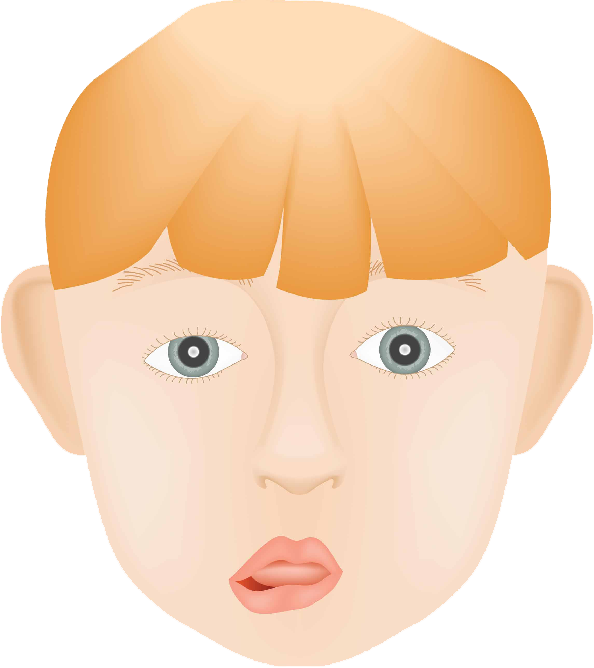
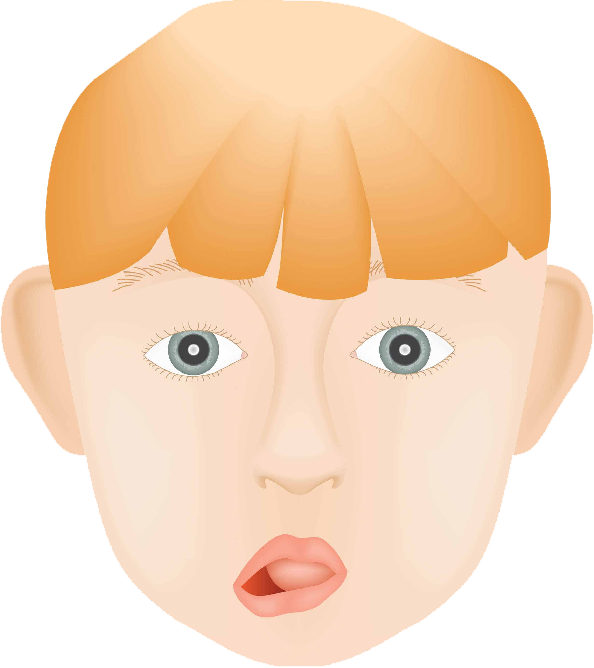
Marcus Gunn jaw-wink ptosis is an example of synkinesis — an abnormal neural connection between two muscle groups that are normally unrelated. A branch of the trigeminal nerve (CN V, which supplies the pterygoid jaw muscles) misdirects into the branch of the oculomotor nerve (CN III) that lifts the upper eyelid. The result: the ptotic lid rises whenever the jaw opens or moves laterally.
Use the slider in the animation above to simulate the jaw-wink synkinesis — the eyelid rising as the jaw opens.
Key Features
- Occurs in 2–13% of patients with congenital ptosis
- Levator function is typically poor (≤ 4 mm)
- Does not improve spontaneously, though children learn to minimize visible jaw movement over time
- Associated strabismus in ≈ 60%, amblyopia in ≈ 35%
Treatment
The surgical approach is guided by the severity of both the ptosis and the jaw-wink:
- Mild jaw-wink with significant ptosis: unilateral frontalis sling may achieve acceptable symmetry
- Significant jaw-wink: bilateral levator muscle disinsertion followed by bilateral frontalis sling — this is intended to abolish the visible wink and allow more symmetric correction
Marcus Gunn jaw-wink is one of several congenital eyelid and orbital conditions present from birth.
Your Surgeon
Thomas C. Spoor, MD, FACS
Michigan Neuro-Ophthalmology & Oculoplastics
🏅 ASOPRS Fellowship Trained